stage
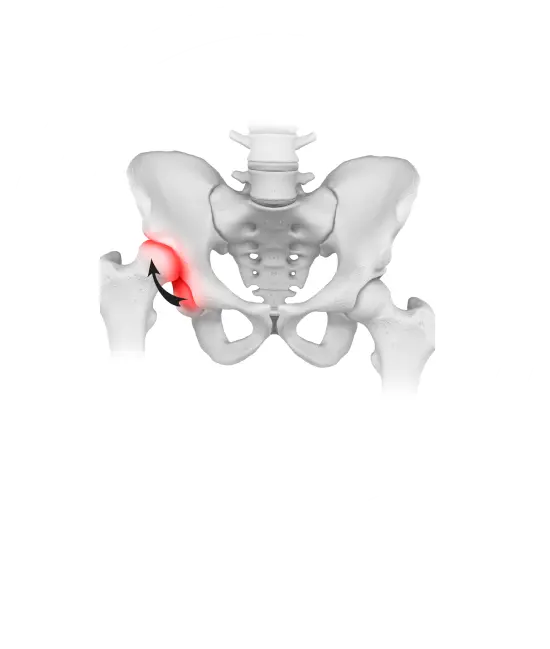
They may have similar clinical symptoms. In the fourth stage of development of hip dysplasia, symptoms and limitation of movements are most pronounced. Pain is constantly present, sharply intensifies at the beginning of movement, bothers the patient more at night. The thigh muscles, pelvic muscles atrophy, the pelvis skews, one leg becomes shorter than the other. The patient wanders when walking — goose gait appears. X-ray shows a significantly deformed joint gap, changes in the bone structure of the femoral head, while with stage 3 dysplasia, the head displacement is 75-100%, and with stage 4, the head displaces by more than 100%. Left-sided, right-sided or bilateral dysplastic coxarthrosis of 3-4 stages leads to persistent impaired motor function and disability.